Knee Problems
Knee problems may include osteoarthritis, ligament injury or cartilage damage. These may require a knee replacement, ligament reconstruction or chondral grafting.
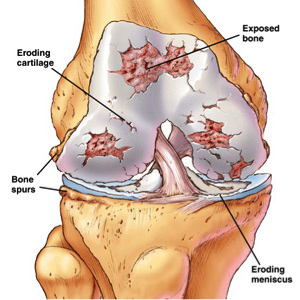
Osteoarthritis of the Knee:
Osteoarthritis of the knee is one of the most common arthritis conditions. These are traditionally described as problems of the ageing population, but these days with more active lifestyles and increasing body weight, it has become an occurrence in young individuals, thereby making it an issue difficult to manage.
The knee joint is a hinge joint and has a sliding and gliding motion. Four to six times your body weight is transferred through your knee when you are standing, walking and running. If your knee is not aligned properly either by birth or due to trauma, a higher percentage of weight transfer occurs through selected areas of the knee causing exaggerated knee wear.
Cartilage wear is irreparable and should be prevented. Maintaining appropriate body weight, regular exercise to strengthen your muscles around the knee and providing nourishment to your cartilage by walking and exercising (cartilage gets nourishment by the pumping of joint fluid into it during walking) are the best ways to provide longevity to your knee joint.
Treating early onset osteoarthritis of the knee:
- Avoid heavy loading activity.
- Perform strengthening exercises to the muscle around the knee. Physiotherapy and hydrotherapy can aid in this.
- Use weight-relieving measures such as using a walking stick or a walking frame.
- Use steroidal and non-steroidal anti-inflammatory medications.
- Use chondro-protective medication supplementation such as Glucosamine and Chondroitin sulphate.
- Occasionally, the use of splints and hot fomentations may provide symptomatic relief. Splints do not provide rigid support but offer a proprioceptive protection.
If these fail, surgical intervention may be of benefit. Arthroscopic debridement of the knee in the elderly population is of limited advantage and offers more risks than benefits, in advanced conditions a total knee replacement may be preferable. In young patients with mechanical symptoms, on the other hand, arthroscopic debridement may be beneficial.
The best pain-relieving operation for end stage osteoarthritis of the knee is a total knee replacement.
What is Total Knee Replacement?
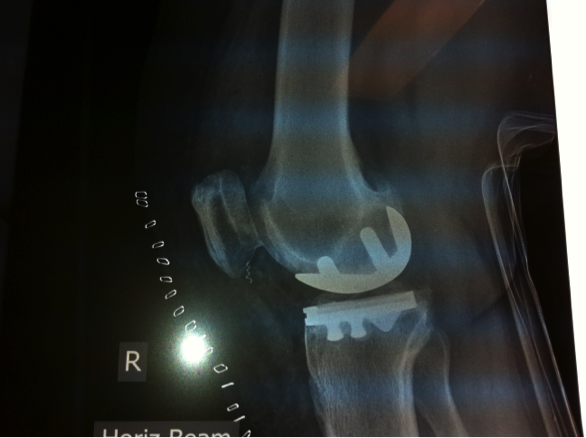
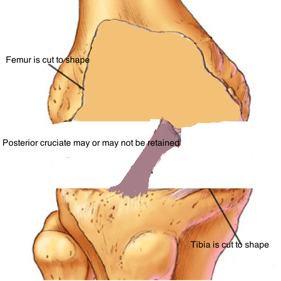
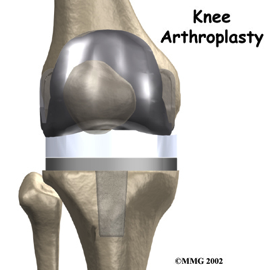
Total knee replacement involves removal of the cartilage in the knee joint along with adjacent bone ends and replacing it with an artificial knee joint made of metal and plastic.
Total knee replacement is universally done through a cut in the skin over the middle of the knee joint. The knee joint is exposed and measured cuts are made through the lower end of thighbone (femur) and the upper end of the leg bone (tibia) using appropriate jigs. In doing so, the diseased cartilage is removed and this is replaced with artificial metal implants, which are then interposed with plastic liners that act like the cartilage.
The success of the knee replacement depends on the tension provided by the artificial implants so that the ligaments on the outside can hold the knee in perfect alignment, allowing the sliding and gliding movements.
Traditional instruments offer 90-95% accuracy for these cutting surfaces. In order to improve the accuracy of these cuts newer cutting systems such as computer-assisted surgery, patient specific instrumentation and robotic surgery are available. These improve the accuracy but the long-term outcome with longevity and function is yet to be recorded.
Mr Unni is able to offer these newer techniques to his patients and he currently utilises patient specific instrumentation for his routine total knee replacements in order to improve accuracy. This, combined with local infiltration of anaesthetics into the knee joint during surgery, creates a pain free post-operative period for the patients.
Post-operative management:
You will begin weight bearing exercises the day after your surgery. The emphasis is on helping you to fully stretch your knee and be able to bend it to at least 90 degrees before you leave the hospital.
Mr Unni has special measures to control pain by local infiltration into the knee joint in order to achieve the movements mentioned above. You will then either be discharged home or to a rehabilitation centre, based on your ability to cope at home. The hospital staff will assist you in this regard.
As any other orthopaedic surgery, total knee replacement is associated with specific complications. There is a 90-95% success rate with knee replacements.
The main complications associated with it are:
- Infection: generally affecting 1% of patients, risk is slightly increased if associated with other co-morbidities.
- Stiffness: There is a risk of not achieving full range of movement, which is more related to a lack of exercise in the early period or history of previous scarring or non-specific pain or infection. If caught early, Mr Unni will organise to rectify this issue to improve the range and thereby achieve full movement in the knee. This procedure carries a small risk of fracture.
- Deep vein thrombosis: Affecting approximately 1% of patients, and very rarely pulmonary embolism (0.02%).
- Neuro-vascular injury: Injury to the nerves around the knee can very rarely occur and may occasionally lead to weakness of the foot, which usually recovers.
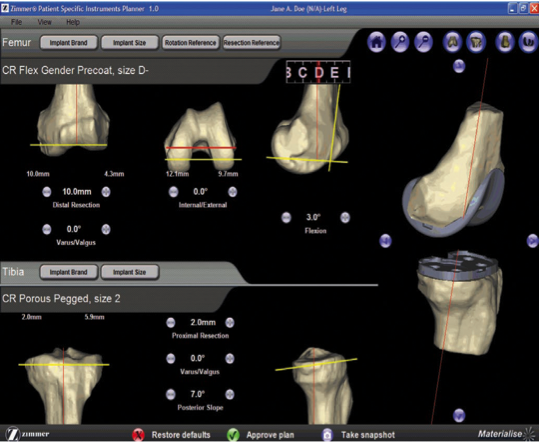
What is patient specific instrumentation in knee replacement?
The traditional knee replacement technique uses instruments that require the surgeon to calculate the angle of cuts. This poses a risk of error a few millimetres away from the normal and can infrequently affect the outcome of the replacement. In order to achieve more perfect alignment, new techniques such as patient specific instrumentation utilise pre-operative MRIs or CT scans to accurately map the shape of the patient’s bones and cartilage. Based on this study, a bone model is created prior to surgery and bone blocks are made and provided during surgery. The bone is then cut during surgery using this bone model. Therefore, not only is time saved but also less invasive measures are utilised and more accurate cuts can be made.
This technique, along with the infiltration of local anaesthetics into the wound during surgery, has reduced the post-operative pain in Mr Unni’s patients and allowed them to mobilise and recover faster.
MRI images from patient being used to calculate the cuts to make to bone models
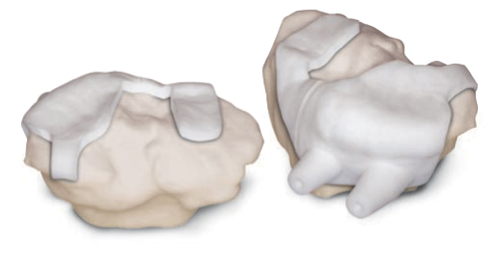
Bone blocks made for use during the operation
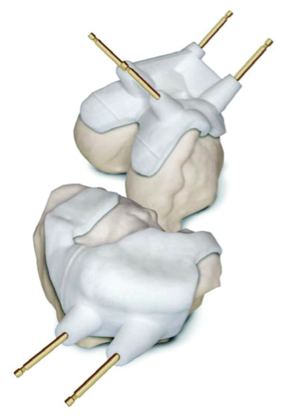
Bone blocks used to pin the bone while cutting it.
Navigated and Robotic Knee replacement
Knee replacement is performed for end stage osteoarthritis and the outcome is looking at pain relief and improving function.
The National Joint Registry, which is an evidence, based registry looking at the outcome of all joint replacement in the country suggest 80 to 90 percent improvement in outcome.
To improve the precision of implant placement more modern technological advancement have been implemented.
This has been available for more than two decades where computer navigation is utilised to map implant position and achieve precision in knee replacement.

This is an extended program of navigated knee replacement, where a Robotic arm is utilised as a super computer to feed facts including the soft tissue tension in the knee to replicate the same in a knee replacement and achieve near anatomical and kinematic replacement of the knee.

Unicompartmental Knee Replacement (partial knee replacement)
What is a unicompartmental knee replacement?
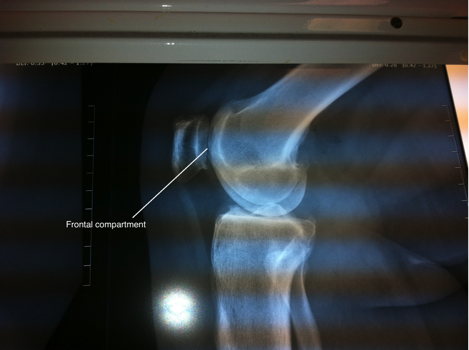
The knee joint has three compartments. These are the medial tibiofemoral (inside) compartment, lateral tibiofemoral (outside) compartment and the patellofemoral (front) compartment. Each compartment has its own lining cartilage and cushioning cartilage. In osteoarthritis, the disease usually starts in one compartment and then gradually spreads to other compartments as it progresses. The medial compartment is often the first to be affected because the body weight is maximally transferred through this compartment. Therefore, in the early stage of the disease this is the first compartment to have damage to its cartilage. The disease often spreads progressively to the other compartments and by the time patients present to their doctor, all three compartments have been affected. Very rarely, only a single compartment is badly damaged, causing the patients isolated pain, while the other compartments still maintain their integrity. In such situations it is possible to replace only the affected compartment and achieve good pain relief.
The outcome of a partial knee replacement (unicompartmental knee replacement) is not as good as a complete knee replacement. It is therefore very important to ensure that only a single compartment is involved, to make sure that a unicompartmental knee replacement would have the best result for the patient. It is important to note that partial knee replacements may require revision to a full knee replacement, an initial complete knee replacement would have a greater longevity than these revised knee replacements.
The advantage of a partial knee replacement is that it is a smaller operation and the recovery is quicker compared to a full knee replacement.
The most common replacement is done in the medial compartment. Replacements for other compartments are not as successful as the medial compartment and the cause of arthritis in these compartments is not purely osteoarthritis, but also inflammation and deformity.
What other treatment modalities can be offered to a patient with unicompartmental osteoarthritis?
The patient may explore non-operative treatment modalities such as relieving the weight with a walking stick or transferring the load to other compartments by using inserts in the shoes, and occasionally injecting steroids into the knee to relieve the pain.
Other surgical treatment options include high tibial osteotomy, which involves breaking the bone and correcting the shape to transfer the load to other compartments, thereby reducing the stress on the affected compartment. This is only performed if the disease is in its early stage. Patients need to be made aware that there can be a cosmetic deformity due to the breaking and realigning of the knee.
Medial (inside compartment arthritis)

Medial compartment replacement